Road to recovery: Cancer in the COVID-19 era
Delays in screening and diagnosis
 Many screening services operated at reduced capacity during the initial waves of the pandemic — in some jurisdictions, up to 40% fewer tests were conducted in 2020 than in 2019 — meaning people were not being screened for certain types of cancer as often or on the same schedule as before COVID-19.1,2 While screening services returned to pre-pandemic levels in 2021, the impacts of those initial delays will be long-lasting.
Many screening services operated at reduced capacity during the initial waves of the pandemic — in some jurisdictions, up to 40% fewer tests were conducted in 2020 than in 2019 — meaning people were not being screened for certain types of cancer as often or on the same schedule as before COVID-19.1,2 While screening services returned to pre-pandemic levels in 2021, the impacts of those initial delays will be long-lasting.
Some populations have been more affected by delays in screening and diagnosis than others. For example, Ontarians who live in lower income neighbourhoods are more likely to experience diagnostic delays following an abnormal breast or colorectal cancer screening test.1 In addition, First Nations peoples living on reserve in Ontario are may be more likely to experience diagnostic delay following an abnormal screening test.1 That means their cancer may be be diagnosed at a later stage when chances of cure and survival are lower.
Primary care providers can play a critical role in the early identification of potential new cases of cancer, but pandemic-related restrictions and service reductions made it harder for many people to see primary care, diagnostic or specialist consult providers in person. Physician activity was well below pre-pandemic levels throughout 2020, which may have resulted in fewer cancers being diagnosed early.3
Canada lagging internationally in some areas
Studies by the International Cancer Benchmarking Partnership (ICBP) have shown that although overall Canada has a high cancer survival rate compared to similar high-income countries, it lags behind for certain cancers, such as esophageal and ovarian cancer.4 In addition, improvements in survival in recent years have not been as pronounced as those of peer countries, which means Canada’s relative standing may be slipping.
The gaps in survival are driven largely by limitations in cancer care capacity. Recent ICBP studies found that Canada ranks below peer countries in access to key diagnostic tools such as PET-CT scanners.5 In 2017, Canada had 0.13 PET-CT scanners per 100,000 people, lower than Australia, Denmark, Ireland and Norway. (The number of scanners reported ranged from 0.04 per 100,000 in Wales to 0.66 per 100,000 in Denmark.)
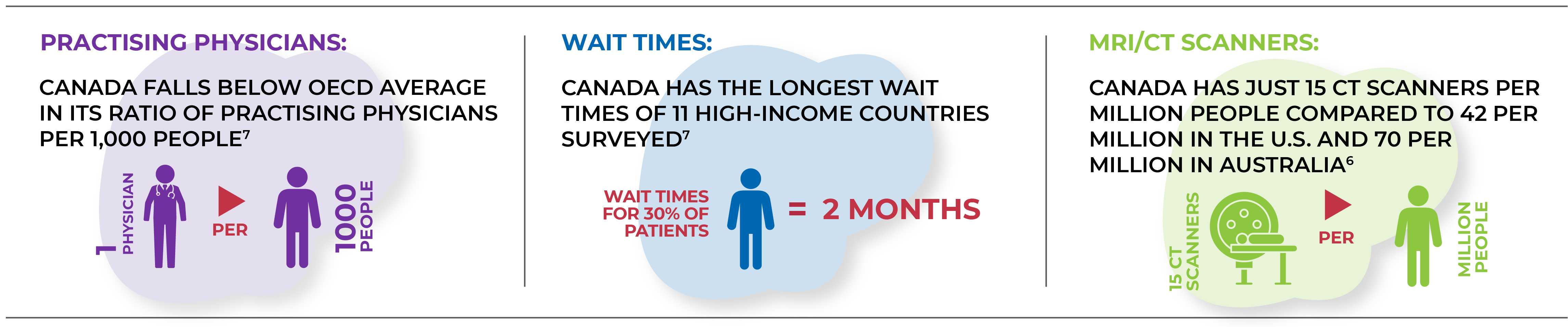
- Practising physicians: Canada falls below OECD average in its ratio of practising physicians per 1,000 people6
- Wait times: Canada has the longest wait times of 11 high-income countries surveyed, with 30% of patients waiting 2+ months for specialist appointments7
- MRI/CT scanners: Canada has just 15 CT scanners per million people compared to 42 per million in the U.S. and 70 per million in Australia6
Other challenges contributing to survival gaps involve pathways to diagnosis. A recent study found that 28% of people in Canada are diagnosed with cancer via emergency hospital admission, which is associated with worse outcomes and a lower likelihood of survival. While Canada had the third-lowest percentage of the nine countries participating in the study — which ranged from 24% to 43% of individuals diagnosed via emergency presentation — there is clear room for improvement in this area.8
Research is underway to contextualize differences in cancer survival in high-income countries and to explore ways to close these gaps in the Canadian context.
- Walker MJ, Meggetto O, Gao J, Espino-Hernandez G, Jembere N, Bravo CA, et al. Measuring the impact of the COVID-19 pandemic on organized cancer screening and diagnostic follow-up care in Ontario, Canada: A provincial, population-based study. Prev Med. 2021; 151:106586.
- Provincial data submission: New Brunswick screening team.
- Canadian Institute for Health Information. COVID-19’s impact on physician services. 2021. Available from: https://www.cihi.ca/en/covid-19-resources/impact-of-covid-19-on-canadas-health-care-systems/physician-services
- Arnold M, Rutherford MJ, Bardot A, Ferlay J, Andersson TM, Myklebust TA, et al. Progress in cancer survival, mortality, and incidence in seven high-income countries 1995–2014 (ICBP SURVMARK-2): a population-based study. Lancet Oncology. 2019; 20(11):1493-1505.
- Lynch C, Reguilon I, Langer DL, Lane D, De P, Wong W-L, et al. A comparative analysis: international variation in PET-CT service provision in oncology-an International Cancer Benchmarking Partnership study. Int J Qual Health Care. 2021; 33(1):mzaa166.
- OECD. Cancer care: Assuring quality to improve survival. 2013. OECD Publishing. Available from: https://data.oecd.org/healtheqt/computed-tomography-ct-scanners.htm
- Commonwealth Fund. 2016 Commonwealth Fund International Health Policy Survey of Adults. 2016. Available from: https://www.commonwealthfund.org/publications/surveys/2016/nov/2016-commonwealth-fund-international-health-policy-survey-adults
- McPhail S, Swann R, Johnson SA, Barclay ME, Elkader HA, Alvi R, et al. Risk factors and prognostic implications of diagnosis of cancer within 30 days after an emergency hospital admission (emergency presentation): an International Cancer Benchmarking Partnership (ICBP) population-based study. Lancet Oncol. 2022 Apr 6; S1470-2045(22)00127-9.